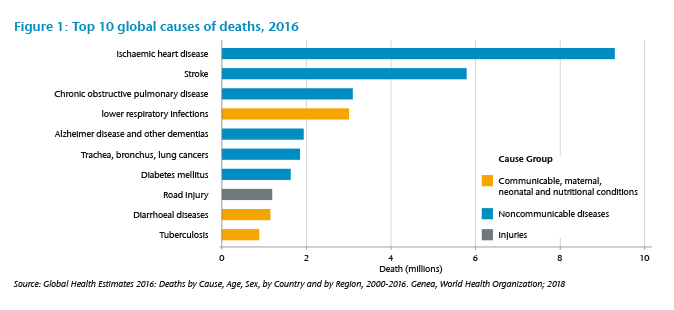
It is well known that cardiovascular diseases, such as heart attacks, are the leading cause of death worldwide. As well as being life-threatening they are also often a warning sign to individuals that can lead to lifestyle changes. It is understandable that the insured, who was diagnosed with a heart attack, expects his Critical Illness (CI) cover to pay a benefit. This, however, might not always be the case, depending on the severity level and the CI definitions.
This expectation has, in some markets, created pressure for insurers to offer CI products based on diagnosis-only definitions. In this case, a benefit is paid for every heart attack diagnosed by a medical professional, irrespective of the severity of the event. But paying each claim resulting from a heart attack is not always in the best interest of all insureds because claims payments that exceed the insurable interest lead to higher than necessary premiums.
We have seen enormous medical progress in the field of cardiovascular disease over the past decades. Treatment of heart attacks has improved to the point where they often cause less harm than they would have done 30 years ago. The Swedish Heart Failure Registry, which conducts detailed analyses of heart attack incidence and mortality annually, found that 365-day mortality after a heart attack has dropped from almost 20% in 1995 to less than 10% for the years 2007 onwards.2
This reduction reflects not only improved treatments but also changes in the detection of heart attacks. With biomarker tests, namely troponin, and more recently high-sensitive troponin, heart attacks can be detected earlier and more accurately than before, resulting in earlier and more precise treatment. Before the introduction of troponin, some heart attacks that did not cause ECG changes or showed unclear changes (NSTEMI) were classified as Angina Pectoris (chest pain).3 Since then, the proportion of full thickness infarctions of the heart (so called STEMI), which are predominantly defined by ECG changes and less by raised troponin levels, has dropped significantly over the past years. The increasing number of diagnosed NSTEMI’s are mainly responsible for this reduction. A higher proportion of – on average – less severe NSTEMI infarctions, better diagnostics and therefore more precise and faster treatment have all contributed to the observed reduction in heart attack mortality. There are now many cases where the pumping function of the heart – the ejection fraction (EF) – is not significantly reduced after a heart attack.
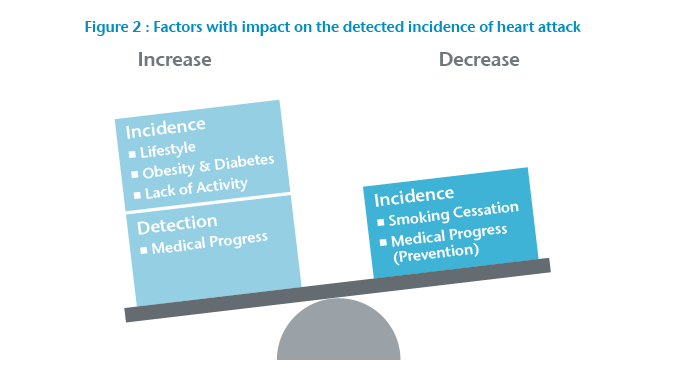
Within the same period, the incidence rate was also observed as stagnating or declining in many countries.4 A major cause of this reduction is likely to be the decline in smokers in these countries. But, the potential gains from smoking cessation are not endless and, in several countries, we see that progress is slowing. Negative effects of the modern lifestyle, with its oversupply of calories and lack of physical activity, weigh heavily against the positive effects from smoking cessation (Figure 2).
“Heart attacks have been and still are a major health threat”
Between 1980 and 2015 the prevalence of obesity more than doubled on a global scale, affecting both developed and developing countries.5 As a result, we observe a pandemic of obesity, hypertension and diabetes posing a major threat to cardiovascular health.
In summary, heart attacks have been and still are a major health threat. The demand for diagnosis-only benefits is understandable, but insuring every claim comes with a high risk of future changes. Outcomes continue to improve, which means that the negative impact on the quality of life after a heart attack will decrease and therefore the necessity for an insurance cover of a heart attack with a very good outcome becomes questionable.
What can be done?
Finding a common denominator between customer expectations and needs is crucial. What does the customer need the product for? In some markets CI cover is used as an add-on for health insurance. In this case, the policy needs to cover all acute heart attacks to provide a reimbursement-like benefit. But even though there is customer demand for the expensive pay-all-diagnoses approach, it is still a risky venture for the insurer, especially with guaranteed business. Here, stepped benefits can help to limit costs for minor events.
In markets where CI is used to cover debt and the long-term lack of income after a severe infarction, a more robust definition can be in the interest of the policyholder as it leads to more affordable rates.
The general product setting is also important. Is it a product with long durations and guaranteed rates? Then the risk of change and its impact on different severity levels in the definitions must be considered. We have the risk of increasing incidence rates due to lifestyle, which affects any definition. There is also a trend toward improved detection of heart attacks, which can lead to more claims for weak definitions only. A further shift to less severe heart attacks could improve outcomes for stricter definitions but would not change the experience for weak definitions. For these reasons, stricter definitions can be preferable for products with long term guarantees.
For a market operating under standard definitions set by the regulator, the potential to change the disease wording itself is limited and the insurer may be required to offer definitions with low to no severity levels. To limit the exposure to certain risk factors, other product features, such as the maximum sum insured or the duration of the contract, can be reduced.
Generally, the insurer should always look for outdated or unclear elements. The best way to ensure that the customer’s expectations match the insurance cover is to have transparent and easy to understand definitions with clearly stated severity requirements for the benefit payment. Ideally, the definitions should be reviewed regularly to depict the changes in medical definitions and treatment standards.
What are possible thresholds?
In some markets, we observe definitions where only STEMI infarctions are covered. This is a clearly defined severity level, but as the proportion of STEMI on all infarctions has decreased significantly in many markets, this may be considered as too restrictive. Also, while STEMI has a significantly higher 30-day-mortality than NSTEMI,6 the long-term effects are similar.7 While STEMI infarctions theoretically pose a transparent severity criterion, the similarity in long-term mortality and symptoms may still result in the customer feeling unfairly treated if he suffers from a severe NSTEMI.
Some definitions use troponin thresholds. These allow, from a medical point of view, for much more detailed differentiation between heart attacks. However, most laymen have hardly ever heard of troponin, let alone understand the implication of different troponin thresholds, so the transparency of such a definition is questionable. The upside of these thresholds are the clear criterion for medical professionals, the downside is the necessity for explanation by a medical professional for policyholders to understand the cover.
Additionally, the time that passes between the heart attack occuring and the measurement of the troponin level will impact the magnitude of the troponin substantially, which makes it even more difficult to use a fixed troponin value as a clear cut off point for a decision about a claim. In the past it was more common to measure serial troponin, which gave a detailed picture of the magnitude of the peak. Nowadays serial troponin is not routinely measured, meaning we only observe an excerpt of the curve, which may or may not be the peak. Hence, good policy wording includes changes in troponin, etc. but does not exclusively use a fixed troponin threshold.
It can be difficult for a claims department to decide whether or not the policyholder has a justified claim for a heart attack. Neither clinical symptoms, nor ECG changes, nor troponin alone can determine a heart attack with certainty. Even if the combination of all three indicates a heart attack, there are still cases where differential diagnoses must be excluded.8 We therefore suggest that to be understood clearly, a definition should differentiate between the attack itself and its sequelae. Wall motion abnormalities or a reduced ejection fraction can be good criteria to differentiate between minor and major heart attacks. Focusing on the long-term outcome of a disease makes it easier to explain why some events are covered and others are not. Policyholders can understand that a permanent and significant loss of heart function requires more financial protection than a minor infarction that allows the policyholder to go on with life as before the event.
“Differentiation between minor and major heart attacks is important”
If the definition contains limitations, it is important that these are communicated transparently and are not hidden in the small print. Only then will the consumer be able to make an educated decision and have the awareness that not every event is covered. This will reduce the number of unjustified claim requests and also the reputational risk for the insurer.
A different picture for surgeries
Heart surgeries, such as coronary artery bypass grafts or heart valve repairs, are often included in CI covers and they, too, are affected by medical progress.